
Clopidogrel (Plavix) – CYP2C19
Rationale
This drug gene interaction (DGI) pertains to the interaction between the cytochrome P450 2C19 (CYP2C19) gene and clopidogrel. Clopidogrel (brand name Plavix®) is used to prevent heart attack and stroke in persons who have recently had a heart attack, stroke, or blood circulation disease (peripheral vascular disease). Clopidogrel works by preventing specific blood cells called platelets from sticking together and forming harmful clots, thus clopidogrel is an ‘antiplatelet drug’ and helps keep blood flowing smoothly in the body. It is also used with aspirin to treat new or worsening chest pain and to prevent blood clots after certain procedures such as a cardiac stent.
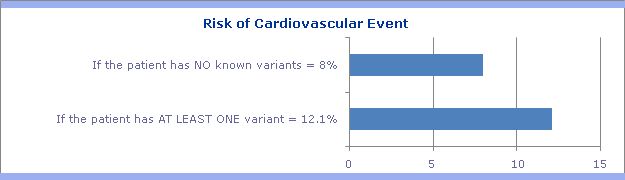
Extensive literature and FDA warning labels indicate patients with genetically reduced CYP2C19 function demonstrate lower systemic exposure to the active metabolite of clopidogrel, diminished anti-platelet responses, and generally exhibit higher cardiovascular event rates following a coronary stent procedure than do patients with normal CYP2C19 function.
Information presented on this page is based on evidence provided by the Clinical Pharmacogenomics Implementation Consortium (CPIC®). CPIC provides peer-reviewed, updated, evidence-based, and freely accessible guidelines for implementing pharmacogenomic results into actionable prescribing decisions for providers. CPIC guidelines include standardized terminology and a systematic grading of evidence and clinical recommendations published in a leading journal (Clinical Pharmacology and Therapeutics).